
Rudra Narayan Saha
Research Scholar
Dr B R Ambedkar National Institute of Technology, Jalandhar, Punjab, India
Email Id – rudenarayansaha37469@gmail.com
1. Introduction
Synthetic polymers are the main reason why soft tissue implants have been so successful. This is mostly because polymers can be made to match the physical and chemical properties of soft tissues. In addition, polymers can be made into different physical forms, such as liquid for filling spaces, fibers for suture materials, films for catheter balloons, knitted fabrics for blood vessel prostheses, and solid forms for cosmetic and weight-bearing uses (PARK, 2011).
The following are minimal requirements for all soft tissue replacements:
1. Close enough estimate of physical properties, especially versatility and feel.
2. The implants shouldn’t break down over time.
3. The implants shouldn’t cause a lot of damage to the tissue.
4. The implants shouldn’t cause thick, fibrous tissue to wrap around or grow into them.
5. The implants should not cause cancer, be safe, not cause allergies, and not cause an immune response.
Other important factors include the ability to be sterilised, the possibility of mass production, the cost, the time it takes to wear out, and the way it looks.
There are two types of Implants:
- Non-Blood Interfacing Implants
(Sutures, surgical tapes, tissue adhesive, maxillofacial implants, artificial skin, eye implants, ear implants, fluid transfer implants, space filling implants etc.)
- Blood Interfacing Implants
(Vascular implants, heart valve implants, heart assist devices etc.)
2. Non blood interfacing implants
2.1 Sutures:
There are two types of sutures, called absorbable and non-absorbable, based on how they behave in the body. They can be told apart by where their raw materials come from: natural sutures (catgut, silk, and cotton) and synthetic ones (nylon, polyethylene, polypropylene, stainless steel, and tantalum). You can also divide sutures into two groups based on how they look: monofilament and multifilament, and there is another which is braided. (Miguel, 2007)
Catgut is a type of absorbable suture that is made of collagen and comes from the inner lining of a sheep’s intestine. Most of the time, it is treated with a chromic salt to make it stronger and slow down its breakdown by cross-linking. With this treatment, the length of time a catgut suture lasts goes from 3–7 days to 20–40 days. (Pillai & Sharma, 2010)
Catgut and other absorbable sutures [nylon, polyglycolic acid (PGA)] cause tissue reactions, but the effect goes away as the sutures are absorbed. This is also true of natural sutures that don’t break down, such as silk
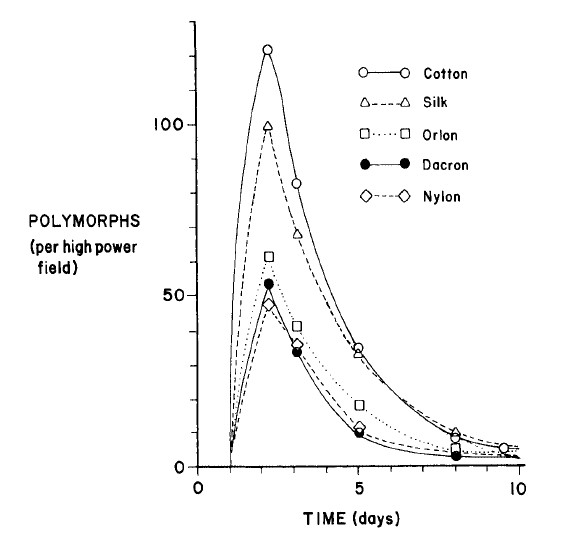
Pic-1: Cellular response to sutured materials (taken from Park, 2011)
and synthetic sutures like polyester, nylon, and polyacrylonitrile cause less reaction than cotton sutures. (Herrmann et al., 1970)
It is worth noting that even minor contamination of the suture increases the risk of infection manifold. The most important factor is the chemical structure and geometric configuration of the suture appear to have no effect on the infection Polypropylene, nylon, and PGA sutures are less prone to infection than stainless steel, plain and chromic catgut, or polyester sutures (Chih-Chang Chu,J. Anthony von Fraunhofer, 1985).
2.2 Surgical tapes:
The use of surgical tapes is supposed to offer a means of avoiding scar tissue formation, problems of stitch abscesses, and tissues that are weakened. The problems with surgical tapes are similar to those with Band-Aids:
(1) misaligned wound edges, (2) poor adhesion due to moisture or dirty wounds, and (3) tape separation when used hematomas, wound drainage, and other complications can occur.
The type of incision used may influence wound strength and scar formation in the skin. The muscles retract if the subcutaneous muscles in the fatty tissue are cut and the overlying skin is taped closed (Yag-Howard, 2014).
When compared to a suture closure, this increases the scar area, resulting in a poor cosmetic appearance. However, due to scar tissue’s greater strength, the taped wound has greater wound strength than the sutured wound only if the muscle was not cut. As a result, despite early studies recommending their use enthusiastically, tapes have not achieved the success that was expected when they were first introduced. Tapes have been successfully used for assembling donor skin scraps for skin grafts, correcting nerve tissues for neural regrowth, and so on.
2.3 Tissue adhesives:
The unique environment of tissues and their ability to heal make it hard to make an ideal tissue adhesive. From what we’ve seen in the past, the best tissue adhesive should be able to stick to wet tissues and be able to polymerize quickly without making too much heat or toxic waste, dissolve as wounds heal without stopping the normal healing process, be easy to prepare for use in the operating room, be able to be sterilised, have a long shelf life, and be easy to make in large quantities.
Covalent bonds between amine, carboxylic acid, and hydroxyl groups in tissues give tissue adhesion most of its strength. There are many types of glue, but alkyl-a-cyanoacrylate is the most well-known. The best alternatives to alkyl-cyanoacrylate are methyl- and ethyl-2-cyanoacrylate. With some plasticizers and fillers. They are called Eastman 910 and Alpha S-2 in the business world, respectively (Yag-Howard, 2014).
Because of the lower strength and lesser predictability of in vivo performance of adhesives, their application is limited to use after trauma on fragile tissues such as spleen, liver, kidney, or after a major surgery of the lung. The use of adhesives on the skin has been mostly successful in plastic surgery and for fixing broken teeth. Just like any other glue, the results of the bond depend on a lot of things, like how thick, porous, and flexible the adhesive film is, as well as how fast it breaks down.
2.4 Percutaneous devices:
The use of artificial kidneys and hearts, as well as the long-term use of injections of drugs and nutrients, has increased the need for percutaneous (trans or through the skin) implants.
The body temperature of people who have been badly burned needs to be kept up as soon as possible. The technology we have now isn’t good enough for biomaterials to actually replace skin. (Saini, 2015)
The main reason it’s hard to get a good connection between the tissue (skin) and an implant (percutaneous) device is because:
A. The tissue can attach to the implant surface at first, but it can’t stay there for a long time because the cells in the dermis are always dying and being replaced by new ones dynamically. Also, the epithelium around the implant either stops growing or grows too much (invagination).
B. Any holes big enough for bacteria to get through will cause an infection, even if the skin and implant were sealed completely at first.
Percutaneous devices are made with a lot of different variables and factors in mind. These things:
End Use factors:
Transmission of information (biopotentials, temperature, pressure, blood flow rate), energy (electrical stimulation, power for heart assist devices), matter (blood cannula), and load (attachment of prosthesis).
Engineering factors:
a. Choosing the materials: polymers, ceramics, metals, and composites.
b. Changing the design: button, tube with and without skirt, porous or smooth surface, etc.
c. Mechanical stress (soft or hard interface, porous or smooth interface)
Biological factors:
a. Humans, dogs, pigs, rabbits, sheep, etc. can be implant hosts.
b. Placement of the implant: abdomen, back, forearm, etc.
Human factors:
a. Care after surgery
b. Implantation method
c. Appearance
2.5 Artificial skins:
An example of a percutaneous implant is artificial skin. Most important for this use is a material that can stick to a large surface.(Burned) surface and keep fluids, electrolytes, and other biomolecules from leaking out until the wound heals. Even though a permanent implant is needed, it is a long way off for the same reasons that percutaneous implants aren’t possible yet. Autografting and homografting are the only permanent solutions that are available right now.
As a burn dressing, reconstituted collagen and a few other polymeric materials have also been tried. Copolymers of vinyl chloride and acetate and methyl-2-cyanoacrylate are two examples. This was found to be too hard and poisonous to be used as a burn dressing. For severe bums the immersion into silicone fluid was found to be beneficial for prevention of early fluid loss, decubitus ulcers and reduction of pain (Park, 2011).
2.6 Maxillofacial implants:
There are two types of materials for maxillofacial implants : extraoral and intraoral.
The latter is defined as follows: “the art and science of anatomical, functional, or structural Cosmetic reconstruction by artificial substitutes of those regions of the maxilla, mandible, and face that are missing or defective due to surgical intervention, trauma, and so on.”
There are many polymeric materials are available for the extraoral implant, which necessitates: (1) Its colour and texture should match that of the patients; (2) it should be mechanically and chemically stable, meaning it should not creep, change colours, or irritate skin; and (3) it should be easily fabricated. Copolymers of polyvinyl chloride and acetate (5-20%), PMMA, silicone, and polyurethane rubbers are currently used (Yaqub Khan et al., 2019).
Because intraoral implants are implanted, the requirements are the same as for other implant materials. A metallic material, such as tantalum or Vitallium, is used to repair maxillary, mandibular, and facial bone defects.To augment soft tissues such as the gums and chin, a polymer such as silicone rubber or PMMA is used. Injectable silicones that polymerize in situ have shown some success in correcting facial deformities. Although this is clearly a better approach in terms of initial surgical damage, it was not accepted due to tissue reaction and eventual implant displacement.
2.7 Ear implants:
Implants can help restore conductive hearing loss caused by otosclerosis (a hereditary defect involving a change in the bony tissue of the ear) and chronic otitis media (middle ear inflammation). There are numerous prostheses available to correct the defects.The porous polyethylene total ossicular replacement implant is used to achieve firm implant fixation through tissue ingrowth. The tilt-top implant is intended to slow tissue ingrowth into the shaft section, which may reduce sound conduction (Park, 2011).
PMMA, PTFE, polyethylene, silicone rubber, stainless steel, and tantalum are have been tested for implant fabrication. Recently, it has been demonstrated that PTFE-carbon composite (Proplast), porous polyethylene (Plastipore), and pyrolytic carbon (Pyrolite) are suitable materials for otology implants.
2.8 Eye implants:
When the cornea and lens are damaged or diseased, eye implants are used to restore their functionality. Since the cornea is usually transplanted from a suitable donor rather than implanted, Because of fixation issues and infection, the cornea implant’s longevity is unknown. The eye implants constructed from “transparent” acrylics, particularly PMMA, which has a high refractive index (1.49). Intraocular lenses have recently gained popularity. As with corneal implants, the major disadvantages of these implants are infection and fixation issues.
There has recently been an attempt to develop an artificial eye for people who have lost all conductive functions of the optic nerve by stimulating brain cells, One of the major challenges with this type of total organ is the development of appropriate electrode materials that will last a long time in vivo without changing their electrochemical properties (Park, 2011).
2.9 Fluid transfer implants
In cases like hydrocephalus and urinary incontinence, you need an implant that moves fluid. Hydrocephalus is caused by an abnormally high level of cerebrospinal fluid pressure in the brain, a cannula is used to pass fluid (mostly ultrafiltrates of blood) through the body. Using implants to fix the urinary system hasn’t worked because it’s hard to connect a fluid-tight prosthesis to a living system. Also, the urine deposits that block the passageway and the constant risk of infection have been hard to deal with.
Many different kinds of material being tested like glass, rubber, silver, tantalum, Vitallium, polyethylene, Dacron, Tefion, and polyvinyl alcohol without much long-term success.
2.10 Space- filling soft tissue implants
Breast implants are a common type of space-filling implant. Breast enlargement was done in the early stages with various materials such as direct injection of paraffin wax, beeswax, or silicone fluids or enclosure in a rubber balloon. Directly injected implants have been linked to a number of issues, including progressive instability and eventual loss of original shape and texture, infection, pain, and so on. Prostheses have been made for people who have had a radical mastectomy or who have deformities that are not symmetrical. Most likely, they are good for you mentally. A prosthesis that is made of silicone gel and polyester mesh so that tissue can grow into it and hold it in place is widely used. Artificial penis, testicles, and vaginas are similar to breast implants (Park, 2011).
3. Blood interfacing implants
There are two types of blood-interfacing implants: short-term extracorporeal implants like membranes for artificial organs (kidney and heart/lung machine) and tubes and catheters for the transport of blood. Implants that stay in place for a long time, like vascular implants and artificial organs that can be put inside the body. Even though heart pacemakers don’t touch blood, they are included here because they are devices that help the blood get to all parts of the body (Park, 2011)
Blood compatibility is the most important thing for implants that connect to blood.
Even though blood clotting is the most important part of blood compatibility, the implants shouldn’t hurt the proteins, enzymes, and other parts of blood that have already formed (red blood cells, white blood cells, and platelets). This includes hemolysis, which is when red blood cells break apart, and the start of the platelet release reaction.
The fundamental requirements for soft tissue implants that interface with blood is the same as for other soft tissue implants, with the exception that the blood-exposed surface must be made non-thrombogenic or at the very least thromboresistant. Most Polymers are used for this type of application because of their flexibility and simplicity of fabrication (Gobbi, 2019).
3.1 Vascular implants
The first material implants were solid tubes made of PMMA, glass, aluminium, gold, and other metals as well as gold and silver. Clots formed in every implant. Porous implants were introduced in the early 1950s, allowing tissue expansion into the interstices. The new tissues’ blood interface reduces clotting. Ironically, thrombogenic materials were found to be more effective for this type of application. Another benefit of tissue ingrowth is the ability to fix the implant by creating a strong anchor from the ingrown tissue. Although the initial leakage through pores is undesirable, this can be avoided by preclotting the implant’s exterior surface before it is implanted. The prosthesis is crimped to stop it from kinking when the implant is bent.
The geometry of fabrics and porosity have a great influence on healing characteristics. The desired porosity is such that 5000 to 10000 ml of water is passed per 1 cm2 of fabric per minute at 120 mm Hg. The lower limit will prevent high leakage of blood and the higher limit is better for tissue ingrowth and healing characteristics. The implant thickness is directly related to the amount of thrombus formation: the thinner the fabric the smaller the thrombus deposit, results faster organization of the neointima.
3.2 Heart valve implants
Similar materials are needed for vascular implants and valve implants. The formed components of blood pressure and flow are some additional requirements. Blood pressure shouldn’t fall below a clinically significant level or become damaged. Valve noise ought to be minimal. Every valve has a sewing ring that is covered with different kinds of polymeric fabrics. This helps when the implant is first put in place. Later, when the tissue grows back, the fixation will still be good, just like the porous vascular implants. Most of the time, the cage is made of metal and covered with fabric to reduce noise or pyrolytic carbon to prevent blood clots.
To help the heart muscles contract regularly, a cardiac pacemaker is used. The electrical impulses that travel through the bundle of His to the atrioventricular (AV) node of the heart are produced by the sinoatrial (SA) node. In the vast majority of cases, pacemakers are used to fix the bundle of His’ conduction issue. In essence, pacemakers should stimulate the heart with a precise amount of electrical stimulation at various heart rates., the pacemaker is made up of conducting electrodes connected to a stimulator.With the exception of the tips, which are sutured or directly embedded into the cardiac wall , the electrodes are well insulated with rubber (typically silicone).
4. Conclusion
In last 3 decades, it is observed that significant advances in the development of biocompatible materials to be used in blood interfacing implants. The dynamics of organ and the resulting mechanical stresses on the formed elements of blood appear to be the main cause for initiation of thrombus. Many further improvements are needed for dynamics and design to minimize the adverse effects of this. Recent advances in the use of minimally invasive grafts also show promise in improving the quality-of-life patients with vascular disease.
5. References
Chih-Chang Chu,J. Anthony von Fraunhofer, H. P. G. (n.d.). Wound Closure Biomaterials and Devices. https://www.ptonline.com/articles/how-to-get-better-mfi-results
Gobbi, S. J. (2019). Requirements for Selection/Development of a Biomaterial. Biomedical Journal of Scientific & Technical Research, 14(3), 1–6. https://doi.org/10.26717/bjstr.2019.14.002554
Herrmann, J. B., Kelly, R. J., & Higgins, G. A. (1970). Polyglycolic Acid Sutures: Laboratory and Clinical Evaluation of a New Absorbable Suture Material. Archives of Surgery, 100(4), 486–490. https://doi.org/10.1001/archsurg.1970.01340220162027
Miguel, F. (2007). * EP001803472A1 *. 1(19), 1–27.
Park, J. B. (2011). Biomaterials science and engineering. http://www.imcdb.lt/courses/regeneraciniu-organizmo-galimybiu-ir-mechanizmu-tyrimai-ir-jais-pagristu-gydymo-technologiju-kurimas/
Pillai, C. K. S., & Sharma, C. P. (2010). Review paper: Absorbable polymeric surgical sutures: Chemistry, production, properties, biodegradability, and performance. Journal of Biomaterials Applications, 25(4), 291–366. https://doi.org/10.1177/0885328210384890
Saini, M. (2015). Implant biomaterials: A comprehensive review. World Journal of Clinical Cases, 3(1), 52. https://doi.org/10.12998/wjcc.v3.i1.52
Yag-Howard, C. (2014). Sutures, needles, and tissue adhesives: A review for dermatologic surgery. Dermatologic Surgery, 40(SUPPL. 9), 3–15. https://doi.org/10.1097/01.DSS.0000452738.23278.2d
Yaqub Khan, M., Mohd Yaqub, K., & Min-Hua, C. (2019). International Journal of Bio-Pharma Research A Review on role of biomaterials in biomedical field. October. https://doi.org/10.21746/ijbpr.2019.8.9.2
About the Author: Rudra Narayan Saha is a graduate of Govt. College of Engg. & Textile Technology, Berhampore, West Bengal, where he earned his degree in Textile Technology. He also holds a Master's degree in Textile Engineering from GCETTB. Rudra N Saha specialises in the education of weaving and textile testing section. He is currently conducting research at NIT Jalandhar, focusing on advancements in medical textiles.